Apicoectomy:
When Microsurgery Saves a Tooth
When a previous root canal can't be retreated through the crown, an apicoectomy approaches the problem from a different angle — literally. Modern microsurgical techniques have made this one of the most predictable ways to save a tooth.
Patient Education
What endodontic surgery actually involves
A short video from the American Association of Endodontists explaining apicoectomy and how endodontic microsurgery saves teeth that didn't fully heal after a root canal.
When Is an Apicoectomy Recommended?
Apicoectomy is recommended when a previously root-canal-treated tooth still shows signs of infection but can't (or shouldn't) be retreated through the crown. Common situations include:
A post is cemented in the root canal and can't be safely removed
The existing crown or bridge is in good condition and shouldn't be disturbed
Infection persists in an accessory canal that can't be reached from inside
Previous retreatment hasn't fully resolved the symptoms
An X-ray shows a persistent dark area at the root tip (apical lesion)
A root tip is fractured or contains a foreign body
The tooth has unusually complex root anatomy
A biopsy of the surrounding tissue is needed
Evidence-based context: indications & how the field has evolved
Apicoectomy is no longer a default response to a failed root canal. Both the standard endodontics textbook and the peer-reviewed literature now describe it as a selective intervention chosen after nonsurgical retreatment has been considered and ruled out.
Accepted clinical indications
Adapted from Morrow & Rubinstein, Endodontic Surgery (Ingle's Endodontics, ch. 12, Table 12-1) — applied in light of current evidence:
- • Failed nonsurgical root canal where retreatment is not feasible (e.g., a well-fitting post, an intact crown that should not be disturbed, or irretrievable filling material)
- • Procedural complications: separated instrument, non-negotiable ledge, root perforation, or symptomatic overfill
- • Anatomic variations that block orthograde access (root dilaceration, apical fenestration)
- • Need for biopsy of a periradicular lesion that does not resolve with conventional treatment
- • Corrective surgery — root-end resection, hemisection, or repair of an external resorptive defect
- • Need for surgical drainage of an acute apical abscess that cannot be drained through the canal
Why the modern procedure looks different
Gutmann's 2014 review in Endodontic Topics (citing Whitehouse, 1884, for the original "rapid picking up of the scalpel" critique) describes the shift from a long-standing over-broad indication list toward today's biologically-grounded, evidence-based decision-making — where nonsurgical revision is considered first, and surgery is reserved for cases where it is genuinely the best option for the patient.
Niemczyk's 2010 review in Dental Clinics of North America documents the parallel adoption of the dental operating microscope (DOM): before 1999, only about half of US endodontists used a microscope; in the cited survey, 97% of endodontists age 35 or younger reported using the DOM for both surgical and nonsurgical treatment. That magnification shift is a major contributor — alongside ultrasonic root-end preparation and biocompatible root-end materials such as MTA — to why modern apicoectomy outcomes (~94%) exceed the older surgical technique's (~59%).
On the choice of root-end material itself, a 2024 randomized controlled trial by Salah et al. in Scientific Reports (56 patients) compared MTA against bioceramic putty (TotalFill) and found no statistically significant difference in periapical healing at 12 months — both achieved high healing rates. Adding a composite bone graft did not change the success rate. In other words, the well-documented modern success of apicoectomy comes from the microsurgical technique (microscope, ultrasonic preparation, a biocompatible seal), not from any single brand of root-end material. This is a small single-center trial, so it is indicative rather than definitive.
Sources: Morrow SG, Rubinstein RA. Endodontic Surgery. In Ingle's Endodontics (ch. 12). · Gutmann JL. Surgical endodontics: past, present, and future. Endod Topics. 2014;30:29–43. · Niemczyk SP. Essentials of endodontic microsurgery. Dent Clin North Am. 2010;54(2):375–399.
How the Procedure Works
A modern apicoectomy is typically completed in a single 60–90 minute appointment under local anesthesia.
Consultation & CBCT 3D Scan
Apicoectomy planning starts with a CBCT 3D scan that maps the exact position of the root tip, sinus, nerves, and surrounding bone. Dr. Kung reviews the scan with you and explains exactly what will happen.
Local Anesthesia
The procedure is done under local anesthesia only — no general sedation needed. The area is fully numbed before any work begins. Most patients report no pain during the procedure.
Microsurgical Access
Under the Zeiss OPMI surgical microscope (up to 25× magnification), Dr. Kung makes a small opening in the gum tissue to access the root tip. Modern microsurgical techniques use much smaller incisions than traditional surgery.
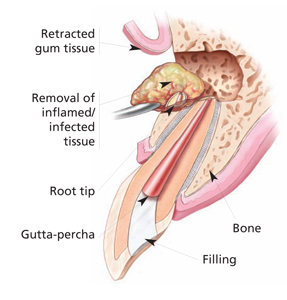
Removing the Infected Tip
Just 2–3 mm of the very end of the root is removed, along with any infected tissue around it. The microscope makes it possible to see the tiny accessory canals at the root tip that often hold the bacteria causing the failure.
Root-End Filling
A small biocompatible filling (typically MTA — mineral trioxide aggregate) is placed in the very tip of the cleaned root to seal it permanently against re-infection. This is the step that makes modern apicoectomy so successful.
Closure & Healing
A few small sutures close the gum tissue. Most patients return to normal activity the next day. Sutures dissolve or are removed at a 1-week follow-up. Bone regenerates over 3–6 months and we verify healing on X-ray.
Recovery & What to Expect
First 24 hours
Some swelling and minor bruising near the surgical site is normal — apply an ice pack for 20-minute intervals. Eat soft foods and avoid the surgical area when chewing. Most patients take ibuprofen for any soreness.
Days 2–7
Swelling resolves over the first week. Most patients return to normal activities, including work, the next day. Avoid vigorous exercise for the first 48 hours. We see you back at one week to remove sutures and check healing.
Weeks 2–8
The gum tissue heals over 2–3 weeks. The bone around the root tip regenerates more slowly. You may notice the area feels normal long before bone healing is complete on X-ray.
3–12 months
Follow-up X-rays at 6 and 12 months confirm bone regeneration. The largest meta-analysis on the subject — 21 studies, more than 1,600 cases — found modern microsurgical apicoectomy succeeds in 94% of cases versus 59% for older traditional techniques. The microscope and modern instruments make the difference. See the research →
Why Modern Microsurgery Is Different
The apicoectomy of 20 years ago was a much larger surgery with a modest success rate. Today's microsurgical approach is fundamentally different — and the outcomes are dramatically better.
Traditional Apicoectomy
- Naked-eye visibility or low-power loupes
- Large bone removal
- Beveled root cut (45°)
- Amalgam root-end filling
- 59% success rate (Setzer 2010)
Modern Microsurgical Approach
- Surgical microscope (up to 25× magnification)
- Minimal bone removal
- Perpendicular root cut (preserves more tooth)
- MTA biocompatible filling
- 94% success rate (Setzer 2010)
Apicoectomy vs. Retreatment vs. Extraction
When a previously-treated tooth becomes painful or develops an infection at the root tip, three options are usually on the table. Here is how they compare side-by-side.
| Factor | Apicoectomy | Nonsurgical Retreatment | Extraction + Implant |
|---|---|---|---|
| Approach | Microsurgical removal of root tip plus bioceramic root-end seal — accessed through the gum. | Existing crown or filling is opened; old root canal material is removed and the canal is re-cleaned and re-sealed. | Tooth is removed; titanium implant placed after bone healing; crown placed on implant. |
| Modern published success rate | ~94% with a surgical microscope (vs. ~59% with traditional 1960s technique). | ~85% when performed by a specialist with microscope and CBCT. | ~93–95% implant survival; success (no peri-implantitis) is lower. |
| Best when | A high-quality crown or post is in place that should not be disturbed; infection sits at the root tip only. | Original treatment missed a canal, was under-instrumented, or coronal leakage allowed re-infection. | Tooth is vertically fractured, non-restorable, or has severe periodontal bone loss. |
| Recovery | 2–3 days mild swelling; most patients work next day. | Same as a first root canal — 1–2 days mild soreness. | 3–7 days after extraction, then 3–6 months osseointegration. |
| Typical fee (specialist, 2026) | $1,800–$2,800. | $1,400–$2,400 (plus crown replacement if needed). | $4,500–$7,500 + possible bone graft. |
| Preserves the natural tooth? | Yes — and preserves the existing crown. | Yes — but the existing crown often has to be replaced. | No. |
Success-rate figures cite Setzer et al. (J Endod 2012) and Tsesis et al. (J Endod 2013) for surgical outcomes; retreatment figures per Friedman et al. (Toronto Study) and, for the contemporary pooled estimate, Sabeti et al., J Endod 2024;50(4):414–433 — see our full breakdown of that 2024 review.
What the research says about saving teeth surgically
The long-term outcome literature on surgical tooth preservation — both apicoectomy and the closely-related root resection / hemisection — converges on a single dominant theme: case selection drives outcome more than the procedure itself.
- Long-term success of surgical tooth preservation ranges from roughly ~68% to ~97% in published 10–15+ year follow-up cohorts, almost entirely depending on patient and tooth selection rather than which surgical technique is used[7],[12]. Older cohorts that took on poorly-selected cases reported about 32–38% loss over a decade[7],[9]; the same procedure in well-selected cases reaches the ~94% modern-microsurgery success rate documented by Setzer (J Endod 2010).
- The strongest predictors of failure are not the surgical technique — they are parafunctional occlusal load, inadequate underlying endodontic treatment, and poorly placed crown margins. Park's 2009 retrospective on 10-year outcomes identified those three factors as the dominant explainers of variation[10]. Klavan's foundational 1975 paper on root amputation in maxillary molars set the original indication/contraindication framework that the field still uses[8].
- When the tooth is a well-selected candidate, saving it can match implant survival: Fugazzotto's same-private-practice comparison of root-resected molars vs. implants in molar positions reported ~96% vs ~97% cumulative survival over up to 15+ years[12]. The honest read of that paper is not that surgery is "better than" an implant — it is that in the right tooth, neither is clearly better, so the conservative natural-tooth option is reasonable.
- The most recent narrative review of surgical endodontic outcomes (Ng & Gulabivala, Int Endod J 2023) pooled decades of data: the periapical healed rate reached 76% in studies from the 2020s (up from 69% across all years), with reported tooth survival of 48–93% after root-end surgery. It confirms the same pattern seen above — pre-operative loss of the buccal plate, the quality of the root-end preparation, the remaining thickness of apical root dentine, and the tooth's restorative status are what drive the result, while root or crown fracture (not the surgery itself) is the leading reason a treated tooth is ultimately lost.[13]
Numbered references [1]–[13] are listed in the Clinical Reference section at the bottom of this page.
Related procedure: when root resection is the right call instead
An apicoectomy treats infection at the very tip of a root. But sometimes the real problem on a multi-rooted molar isn't the root tip — it's one entire root. A vertical fracture confined to one root, a furcation perforation that can't be repaired from inside, or severe periodontal bone loss isolated to a single root all share the same property: the rest of the tooth is sound, and the cleanest fix is to remove the problem root rather than try to apicect it or extract the whole tooth.
That procedure is called root resection (on a maxillary molar) or hemisection (on a mandibular molar). Oh's 2012 case report in the Journal of Endodontics[11] is the canonical example: combined endodontic-periodontal lesions on the mesiobuccal root of maxillary molars, treated by resecting that single root while preserving the rest of the tooth and its crown. The retained roots received conventional root canal treatment and the tooth stayed in function.
Candidacy for root resection is narrower than candidacy for apicoectomy — it requires the other roots to be endodontically and periodontally sound, with adequate interradicular bone — but in the right tooth it's more conservative than either apicoectomy on the wrong root or extraction-and-implant. Our patient guide walks through the candidacy criteria, realistic 10-year outcomes (Langer 1981[7], Bühler 1988[9]), and how the procedure compares to a molar implant[12].
Read the full guide to root resection & hemisectionFrequently Asked Questions
What is an apicoectomy?
An apicoectomy is a minor surgical procedure that removes the very tip of a tooth's root and any infected tissue around it. It's used to save a tooth when a previous root canal hasn't fully healed and conventional retreatment isn't feasible.
Is an apicoectomy painful?
No. The procedure is done under local anesthesia, and most patients report no pain during the surgery itself. Mild soreness and minor swelling for 1–3 days afterward is normal and typically managed with over-the-counter ibuprofen.
What's the success rate?
The largest meta-analysis on the subject — 21 studies and over 1,600 cases — found that modern endodontic microsurgery succeeds in 94% of cases at one year or longer (Setzer FC et al., Journal of Endodontics 2010). The same study found older traditional techniques succeed in only 59% of cases. The difference is statistically significant at p < 0.0005.
How long does recovery take?
Most patients return to normal activities the next day. Sutures are removed or dissolve within a week. The bone around the root tip regenerates over 3–6 months, and full healing is verified by follow-up X-rays.
Will my tooth feel different afterward?
No. After healing, your tooth will function exactly as it did before. Removing 2–3 mm from the root tip does not affect the tooth's stability — the rest of the root and the crown remain fully intact.
How much does an apicoectomy cost?
Cost depends on the tooth and the complexity of the case. We verify your insurance benefits before treatment and provide a written estimate so there are no surprises. See our Insurance & Billing page for how we estimate cost.
When is root resection a better option than an apicoectomy?
When the problem is confined to one root of a multi-rooted molar — for example, a vertical fracture, furcation perforation, or severe localized bone loss on a single root — removing that one root (root resection) can be more conservative than apicoectomy, and far more conservative than extracting the whole tooth and placing an implant. Oh (J Endod 2012)[11] describes mesiobuccal-root resections that preserved otherwise sound maxillary molars as the canonical example. The other roots must be endodontically sound and periodontally supported, with adequate interradicular bone. See our patient guide to root resection and hemisection for the full candidacy criteria.
Further reading
- · Research & Evidence — outcome data behind microsurgery
- · Clinical Protocols & Case Evidence — for dental students and referring doctors
- · Microsurgery vs. traditional surgery: 94% vs 59%
- · How an apicoectomy actually works, step by step
- · What is an apicoectomy and when is it needed?
- · Why magnification matters most for molars
Wondering whether your case actually needs surgery? When is an apicoectomy needed?
Apicoectomy (endodontic microsurgery) — serving 30+ Bay Area cities
Dr. Jason Kung provides apicoectomy (endodontic microsurgery) to patients across Silicon Valley from our Sunnyvale office. Evening and weekend hours, same-day emergencies, free on-site parking.
Financial-bias disclosure: Dr. Kung has no financial relationship — paid consulting, royalty, equity, or promotional — with any implant system, surgical-material manufacturer, or laboratory. The candidacy criteria, success ranges, and comparison to alternative options on this page reflect the published evidence, not a product preference.
Considering Microsurgery?
Bring your previous X-rays. Dr. Kung will do a thorough evaluation, take a CBCT 3D scan if appropriate, and tell you honestly whether microsurgery is the right next step for your tooth.
Mon–Fri 8am–7pm · Sat–Sun 8am–3pm
See also: can a failed root canal be redone? · Saturday apicoectomy scheduling · when is apicoectomy needed? · root resection & hemisection
Related Articles
What to Expect
How an Apicoectomy Actually Works, From the Surgeon's Chair
If your dentist mentions an apicoectomy, the procedure can sound far more intimidating than it actually is. Here's exactly what happens in the room — drawn from the same step-by-step protocol that endodontic residents learn in school and that Dr. Kung uses for every surgical case.
ReadProcedures
The Microscope Effect: Why Magnification Matters Most for Molars
When researchers compared modern apicoectomy outcomes with and without a high-power surgical microscope, the overall difference was 88% vs. 94%. But for molars — the teeth that are hardest to reach, hardest to save, and most expensive to replace — the gap was statistically significant in a way it wasn't for the front teeth.
ReadProcedures
Endodontic Microsurgery vs. Traditional Apicoectomy: 94% Success vs. 59%
If your dentist has mentioned an apicoectomy, the technique used matters far more than most patients realize. The largest meta-analysis on the subject found that endodontic microsurgery succeeds in 94% of cases — compared to 59% with traditional surgical methods still common in oral surgery offices.
Read