The Oldest Root Canal Is 59,000 Years Old — and It Was Performed by a Neanderthal
How did researchers prove a 59,000-year-old Neanderthal molar from Siberia holds the oldest known root canal — and why did the patient survive? An endodontist explains.
By Dr. Jason Kung, DDS, MS — Specialist Endodontist · UCLA DDS · OHSU MS
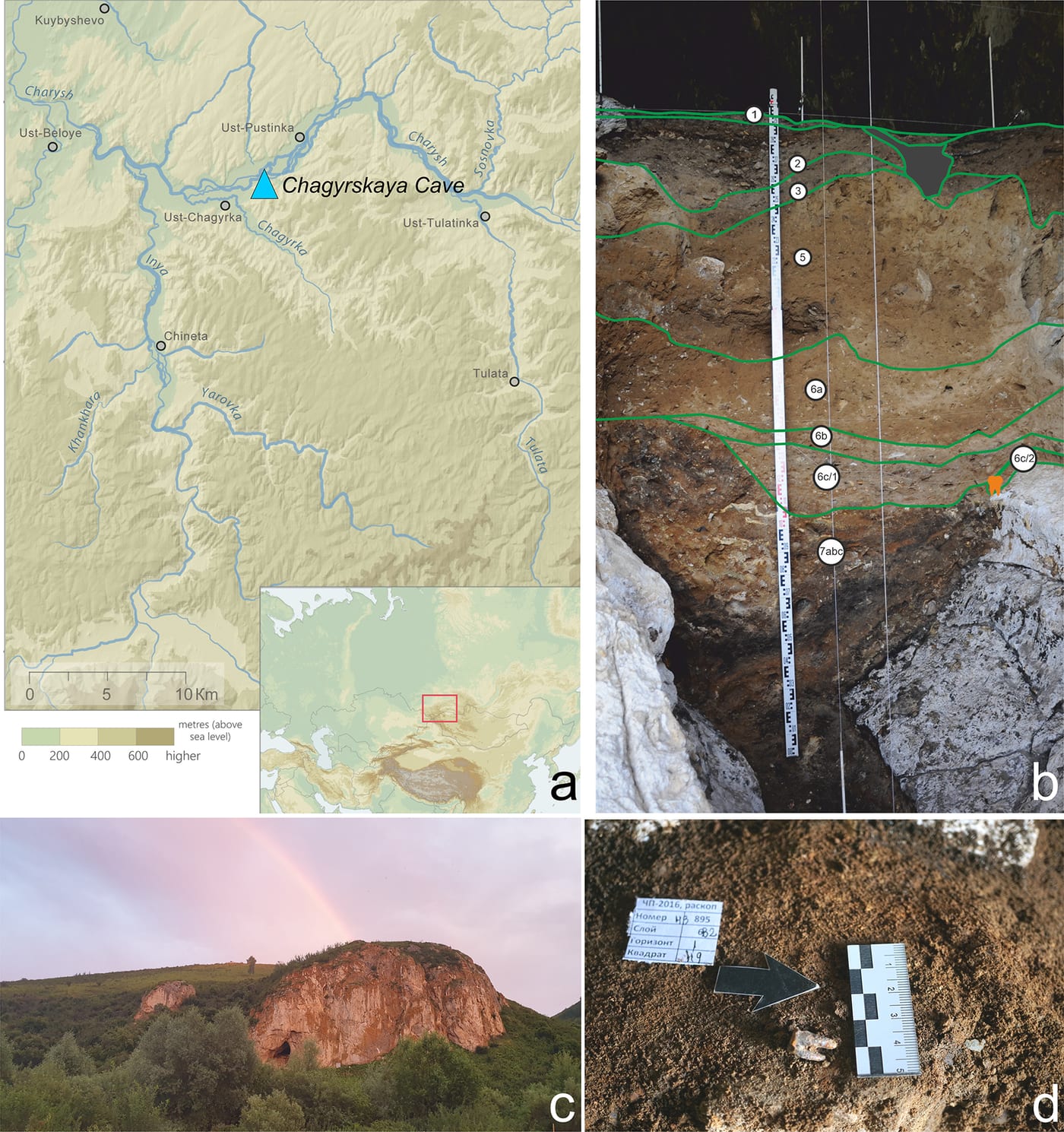
On May 13, 2026, the open-access journal PLOS ONE published a paper with a title that ought to stop any endodontist mid-coffee: Earliest evidence for invasive mitigation of dental caries by Neanderthals (Zubova et al., 2026). The paper describes a single Neanderthal molar — catalogued Chagyrskaya 64 — recovered from Chagyrskaya Cave in the Altai Mountains of southwestern Siberia. The tooth is approximately 59,000 years old. On its biting surface is a small, deliberately drilled cavity that opens into the dental pulp chamber.
In other words, the oldest known root canal access cavity in the archaeological record was made by a Neanderthal, with a stone tool, roughly 30,000 years before our species reached northern Asia.
That is an extraordinary claim, and the research team handled it with appropriate caution. So before getting to what this means for patients sitting in a modern endodontic chair, it is worth walking through what the evidence actually shows — and what it does not.
What the researchers found
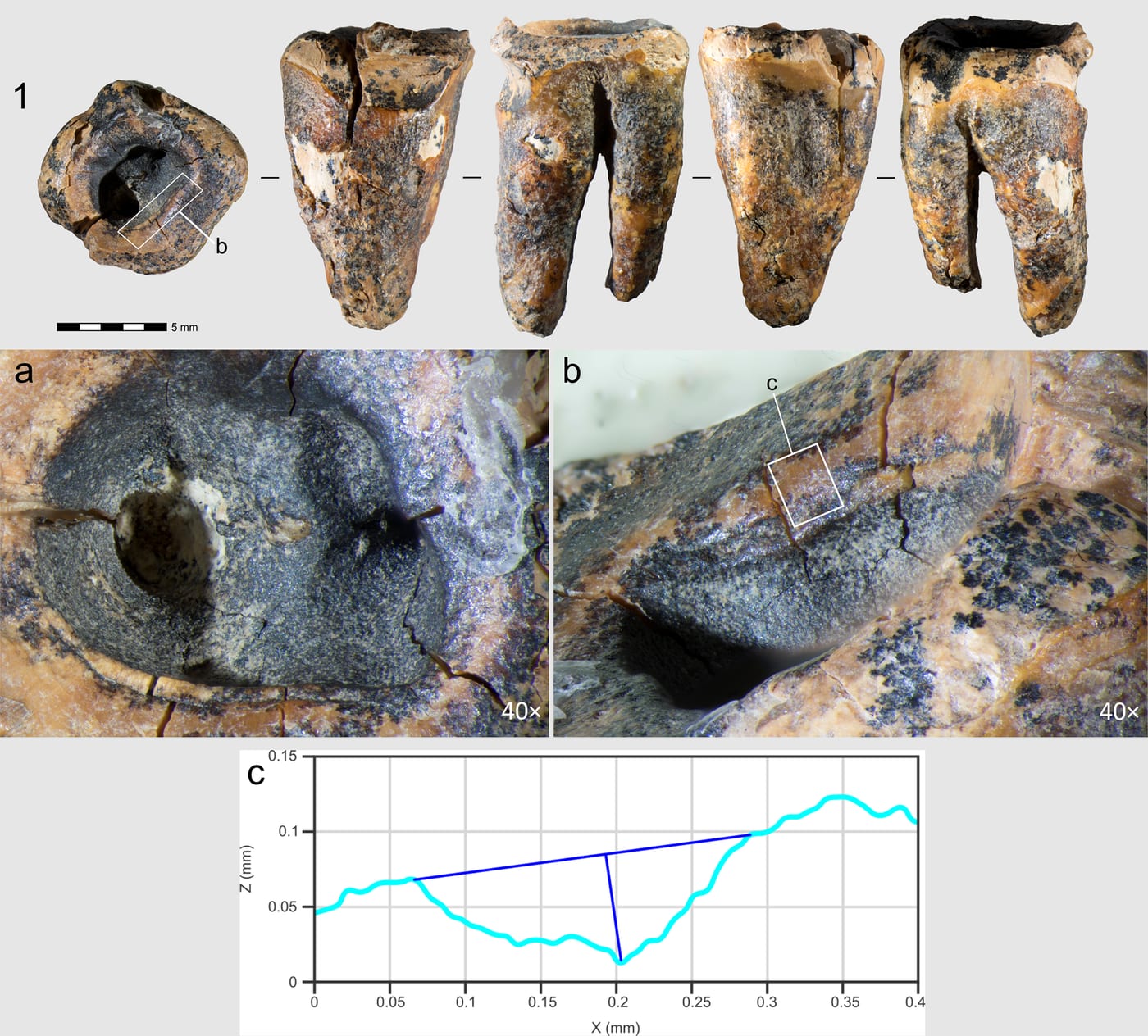
Chagyrskaya 64 is a lower-left second molar from an adult Neanderthal. It was excavated from a well-dated Middle Paleolithic layer of Chagyrskaya Cave, a site already famous for producing high-coverage Neanderthal genomes. The tooth shows three separate kinds of modification on its occlusal (biting) surface:
- A pre-existing carious lesion. The tooth had a real cavity — bacterial decay, not a manufacturing artifact of fossilization.
- Toothpick grooves along the side of the tooth. Toothpick grooves are well-documented in Neanderthal and early modern human teeth and almost certainly represent attempts to dislodge trapped food or relieve gum discomfort.
- A small, roughly cylindrical access cavity drilled directly into the occlusal surface above the carious lesion, extending into the pulp chamber. This is the feature that has not been seen before in a hominin fossil.
How they ruled out the boring explanations
The interesting question is not whether there is a hole, but how it got there. Researchers have to rule out several less remarkable possibilities before claiming a deliberate procedure: post-depositional damage from sediment pressure, animal gnawing, natural wear from chewing hard objects, accidental fracture, and modern excavation damage. The Zubova team addressed each of these systematically:
- Micro-CT scanning. A high-resolution 3D reconstruction of the internal structure of the tooth showed that the access cavity has a consistent, intentional geometry — not the irregular shape of a fracture or the rounded surface of normal wear.
- Traceological (use-wear) analysis. Under scanning electron microscopy, the walls of the access cavity show parallel, semi-circular micro-grooves consistent with a tool being rotated against the dentin under controlled pressure. Natural wear and animal gnawing produce different micro-patterns.
- Experimental replication. The team replicated the procedure on modern human teeth using stone-tool replicas of the kind found at Chagyrskaya. The micro-wear pattern produced by their replica tools matched the pattern on Chagyrskaya 64.
- Survival evidence. Critically, the rim of the drilled cavity shows subsequent chewing wear — meaning the Neanderthal survived the procedure and continued using the tooth afterward. A post-mortem hole would have no such wear pattern.
The paper's conclusion is carefully worded. The authors do not claim that Neanderthals performed root canals in the modern endodontic sense — sealing the canal with an inert filling material, for example, is well outside what they describe. What they argue is that the access cavity represents a deliberate therapeutic intervention beyond palliative care: a planned, invasive procedure to access and debride the carious portion of the pulp chamber, presumably to relieve pain or contain an infection.
What this tells us — and what it doesn't
The temptation is to imagine a Neanderthal "dentist" in a fur cloak working on a patient by firelight. The evidence does not go that far. We have one tooth, from one individual, at one site. We cannot tell whether this was a rare, one-off act of desperation or part of a wider tradition. We also cannot infer who performed the procedure — the Neanderthal in question may have worked on their own tooth, or someone else may have done it for them.
What we can reasonably infer is that the cognitive prerequisites for the act were present in this population: the recognition that pain was coming from a specific tooth, the inference that the bad part of the tooth could be physically removed to help, the dexterity to operate a stone perforator inside another person's (or one's own) mouth, and the tolerance — by whoever was on the receiving end — to sit through it. None of these capacities, individually, is surprising in Neanderthals; we have ample evidence of complex tool use, of care for sick or injured group members, and of medicinal plant use. But the combination, applied to a specific tooth, is new.
The 59,000-year throughline
For those of us who do this work for a living, the most striking thing about Chagyrskaya 64 is how recognizable the basic idea is. The instinct that a sick tooth can be saved — rather than simply pulled or endured — turns out to be very old. The tools have changed almost beyond recognition: a flaked stone perforator becomes a 0.06 mm nickel-titanium rotary file under a surgical microscope. The disinfection has gone from nothing at all to sodium hypochlorite irrigation with ultrasonic activation. The pain control has gone from gritted teeth to profound local anesthesia delivered intraosseously when needed (which is why the answer to "does a root canal hurt?" is, for modern endodontic care, essentially "no"). But the underlying judgment — this tooth is worth saving — is the same judgment a referring dentist makes today when they pick up the phone.
It is also worth noting how much the diagnostic side has changed. The Zubova team needed micro-CT, scanning electron microscopy, and experimental archaeology to confirm what a single tooth was telling them. Modern endodontic diagnosis uses a clinically appropriate cousin of those same tools: cone-beam CT imaging is now standard for retreatment cases, suspected fractures, and complex anatomy. Without 3D imaging, an endodontist is doing what the Neanderthal had to do: working with incomplete information about what is inside the tooth. With it, the work becomes deliberate in the way Chagyrskaya 64 hints at — but with about 59,000 years of accumulated craft behind every decision.
One honest caveat
This is a single fossil, freshly published in May 2026. Other dental anthropologists will examine it, attempt their own replications, and propose alternative interpretations. That is how the literature works, and a finding this striking will (and should) attract that scrutiny. The Zubova team's case is methodologically careful, and the experimental replication is the strongest part. But as with any single-specimen claim in human evolutionary science, the right posture is interested confidence, not certainty. The cautious phrasing in the paper — "earliest evidence for" rather than "first example of" — reflects that the authors know what is at stake.
Why a Cupertino endodontist is writing about a Siberian Neanderthal
Two reasons. The first is just human interest: every endodontist I know spent the morning the paper dropped reading it instead of catching up on charts. The second is that patients, very reasonably, sometimes wonder whether saving a tooth with a root canal is some elaborate modern overreach when the simpler alternative is extraction. The answer — long before specialty training, long before microscopes, long before any of the tools we now take for granted — appears to be that humans (and at least one Neanderthal) have always tried to keep their teeth when they could. Modern endodontic treatment is the latest, by far the most successful, version of a very old impulse.
If you have a tooth that is hurting and you want to know whether it can be saved, that question is exactly the one Dr. Jason Kung sees patients about every day. Learn how a modern root canal actually works, or book an appointment — call (669) 234-2354. The tools are better now.
Have a question about your tooth?
Dr. Kung sees emergency cases the same day when possible. Most consultations are 30 minutes and include a microscope examination.
Related Articles
Research
A Liquid That Stops Cavities Without Drilling? What the 2026 SDF Trial Really Showed
Headlines in July 2026 announced a liquid that stops cavities in seconds, no drill required. The study behind them — a Phase III U.S. trial of silver diamine fluoride in 830 young children — is real and important. Here is what SDF actually does, who it helps, and why it does not change what happens once decay reaches the nerve.
ReadResearch
Why Dentists Are Prescribing Fewer Antibiotics for Tooth Infections — and Why That's Good News
In April 2026 the California Dental Association re-shared the profession's antibiotic-prescribing guidelines alongside a national investigative series asking why inappropriate antibiotic prescribing is still common in dentistry. The encouraging headline: dental clindamycin prescriptions dropped 35% between 2020 and 2025 as dentists embrace stewardship. Here is what the ADA's evidence-based guideline actually says, why 'a course of antibiotics first' is usually the wrong plan for an infected tooth, and what resolves the infection instead.
ReadResearch
Your Mouth and Your Whole-Body Health: Where Tooth Infections Fit Into the Picture
A July 2026 Wall Street Journal report captured a shift underway in medicine: researchers are treating the mouth as a source of bodywide inflammation, linking diseased gums to heart disease, diabetes, Alzheimer's, and more. Most of that research is about gum disease — but the same principle applies to a chronic infection at the root of a tooth, which is exactly what a root canal eliminates. Here is an endodontist's read on what the science does and does not say, and why clearing a silent tooth infection is a whole-body health decision, not just a dental one.
ReadContinue with Dr. Kung
Treatment Guide
Root Canal Treatment with Dr. Kung
How a specialist endodontist performs root canal treatment under the surgical microscope — with comfort, precision, and a 90%+ long-term success rate.
Read the guideSpecialist Consult
Get a Second Opinion
Been told you need an extraction, retreatment, or apicoectomy? A specialist consultation often surfaces options your general dentist could not see.
Schedule a consult