Root Canal Retreatment:
Saving a Tooth That's Failed Once
A root canal that's still painful — even years later — can usually be saved. Retreatment finds what the first procedure missed and gives your tooth a second chance.
Patient Education
What is retreatment, exactly?
A short video from the American Association of Endodontists explaining when a previously treated tooth can be saved with retreatment.
When Is Retreatment Needed?
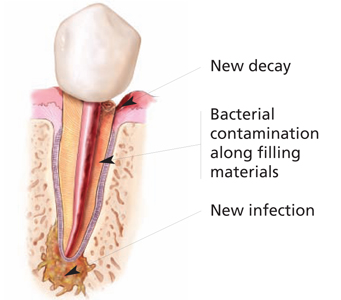
A previously root-canal-treated tooth can develop new symptoms months or even years after the original treatment. Common signs include:
Returning pain in a previously treated tooth
Tenderness or pressure when biting
A pimple or bump on the gum near the tooth
Visible swelling or facial tenderness
A dark spot showing on the X-ray at the root tip
New decay around the existing crown or filling
A cracked or loose crown exposing the tooth
Persistent dull ache that comes and goes
Sometimes a failing root canal causes no symptoms and is only discovered on a routine X-ray. Either way, the sooner it's addressed, the more predictable the outcome.
How Retreatment Works
Most retreatments are completed in one or two visits, depending on complexity.
Comprehensive Re-evaluation
We review your previous treatment records, take new digital X-rays, and almost always perform a CBCT 3D scan to identify exactly why the original treatment failed — missed canals, fractures, persistent infection, or coronal leakage.
Removing Previous Filling Material
Under the Zeiss OPMI surgical microscope, Dr. Kung carefully removes the old gutta-percha and any posts or restorative material blocking access to the canals. This is the most technically demanding step and is where specialist training matters most.
Locating Missed Anatomy
Many failed root canals fail because a small accessory canal was missed in the original treatment. Microscope magnification (up to 25×) lets Dr. Kung find canals that are invisible to the naked eye.
Disinfection & Re-shaping
Each canal is re-cleaned and re-shaped with modern rotary files and irrigated with antimicrobial solutions to eliminate bacteria that survived the first treatment.
Re-sealing
The canals are filled with fresh gutta-percha and sealed with a biocompatible material. A temporary or permanent filling closes the access opening.
Follow-up & Healing Verification
We see you back at 6 and 12 months to verify healing on X-ray. Around 80–90% of retreatments are successful when performed under microscope by a specialist.
Retreatment vs. Apicoectomy vs. Extraction
When a previous root canal hasn't healed properly, you have three options. Saving the tooth — through retreatment first, then microsurgery if needed — is almost always the best long-term choice.
Retreatment (first choice)
- Non-surgical
- 80–90% success rate
- 1–2 appointments
- Saves your natural tooth
Apicoectomy (second choice)
- Microsurgical
- 75–90% success rate
- Single appointment
- Used when retreatment isn't possible
Extraction (last resort)
- Removes the tooth entirely
- Requires implant or bridge to replace
- Higher total cost
- Loss of natural bone over time
Frequently Asked Questions
Why do root canals fail?
The most common reasons are: a missed accessory canal in the original treatment, new decay or a cracked crown allowing bacteria back in, a tooth fracture, or a persistent infection that didn't fully resolve. CBCT 3D imaging usually reveals which of these is the cause.
Is retreatment painful?
No. The tooth is fully numb during the procedure, and most patients describe the experience as similar to the original root canal — pressure but no sharp pain. Some mild soreness for 1–3 days afterward is normal.
What's the success rate of retreatment?
Around 80–90% when performed by a specialist using a surgical microscope. If retreatment isn't appropriate or doesn't fully resolve the problem, endodontic microsurgery (apicoectomy) is the next option and saves an additional ~75–90% of cases.
How much does retreatment cost?
Retreatment typically costs more than a first-time root canal because it's more technically complex. With PPO insurance, expect $400–$900 out-of-pocket. Without insurance, $1,200–$2,000. We provide a full estimate before treatment and verify your insurance benefits.
Should I just have the tooth pulled?
Almost always, saving your natural tooth is the better choice. Even retreatment plus a new crown is typically less expensive than extraction plus an implant, and your natural tooth root preserves jawbone in a way no implant can fully replicate.
Further reading
Based on the research
Saving the natural tooth has measurable long-term advantages.
Setzer & Kim, Journal of Dental Research 2014 — critical review comparing implants and endodontically treated teeth.
Industry-funded implant studies report rosier outcomes than independent ones (63% don't disclose funding; 66% have meaningful bias risk). When a tooth is restorable, retreatment — including microsurgery if needed — keeps your natural bite and avoids the 16–28% peri-implantitis rates seen with implants at 5-year follow-up.
See the researchWhat the 2024 evidence says
78–87% pooled success in contemporary nonsurgical retreatment
A 2024 systematic review in the Journal of Endodontics (Sabeti et al.) restricted its analysis to 29 contemporary studies of nonsurgical retreatment performed with modern tools (nickel-titanium rotary instrumentation, apex locators, digital and CBCT imaging, magnification) and at least two years of follow-up. Pooled periapical healing rates were 78.8% (strict criteria) and 87.5% (loose criteria); pooled overall success was 78.0% and 86.4%. Outcomes were significantly better when the preoperative lesion was small or absent, when the root filling reached within 0–2 mm of the apex, and with longer follow-up.[1]
Those pooled numbers hold up in long-term real-world practice. A 2026 Journal of Endodontics retrospective cohort followed 241 non-surgical retreatments performed by a single clinician over more than three decades, with a median follow-up beyond nine years: radiographic periapical healing exceeded 64%, tooth survival was favorable, and — notably — success rates improved over time as technique and instrumentation advanced. It is a single-operator cohort rather than a controlled trial, but it is among the longest real-world follow-ups published and mirrors what we see from disciplined, specialist-level retreatment.[7]
Modern disinfection refinements can push those numbers higher still. A 2024 Journal of Endodontics retrospective cohort of 120 teeth with stubborn, persistent infection after a prior root canal reported 92.5% success at a mean 30-month follow-up when retreatment combined foraminal enlargement with a 2% chlorhexidine gel — evidence that a well-executed retreatment can be an effective alternative to pulling the tooth. As a single-center retrospective study it is indicative rather than definitive, but it aligns with the pooled data above.[8]
A comprehensive 2023 review of what actually drives endodontic outcomes (Gulabivala & Ng, Int Endod J) reframes the picture: healing is dominated by pre-operative factors — the patient's own biology and the nature and extent of the existing infection — more than by any single technical step. It also explains why retreatment carries a slightly lower chance of healing than a first-time root canal: previous treatment can block access to the fine apical anatomy where residual infection hides, and it alters the host–bacteria balance the retreatment has to overcome. This is precisely why a specialist's magnification, 3D imaging, and disinfection matter most in retreatment cases.[5]
Choosing between non-surgical retreatment and microsurgery is such a nuanced decision that it has become a frontier for artificial intelligence: a 2026 Journal of Endodontics scoping review of AI prognostic models found that while machine learning shows promise in predicting outcomes, no model yet matches a specialist's case-by-case judgment — the decision still hinges on the same clinical factors (lesion size, root anatomy, restorability, prior treatment quality) that Dr. Kung evaluates with CBCT 3D imaging at your consultation.[6]
When non-surgical retreatment is not feasible, endodontic microsurgery (apicoectomy) is the documented surgical alternative, with modern micro-surgical technique reporting substantially higher success than older root-end approaches.[2] Every step described here follows the standard of care set out in the AAE Guide to Clinical Endodontics.[3]
Sabeti M, Chung YJ, Aghamohammadi N, Khansari A, Pakzad R, Azarpazhooh A. J Endod. 2024;50(4):414–433.
Read Dr. Kung's full breakdownRoot canal retreatment — serving 30+ Bay Area cities
Dr. Jason Kung provides root canal retreatment to patients across Silicon Valley from our Sunnyvale office. Evening and weekend hours, same-day emergencies, free on-site parking.
Have a Failing Root Canal?
Bring your previous X-rays if you have them. We'll do a thorough evaluation and tell you honestly what your options are — including whether the tooth can be saved.
Mon–Fri 8am–7pm · Sat–Sun 8am–3pm
See also: Can a failed root canal be redone? · Bay Area failed-root-canal second opinions · weekend microsurgery · tooth resorption
Related Articles
Research
17 Years, 7,340 Root Canals: What a New JOE Study Says About Long-Term Success
The July 2026 issue of the Journal of Endodontics published one of the longest-running root canal outcome studies ever: 7,340 root canals tracked in a single institution from 2008 to 2025. The headline numbers are reassuring — but the study's most practical lesson is about what happens in the weeks after your root canal appointment.
ReadPatient Education
Can One Bad Root Mean Losing the Whole Tooth? Not Always.
Molars have two or three roots, and sometimes only one of them is the problem. Root resection and hemisection are decades-old procedures that remove the failing root and keep the rest of the tooth in function — often for 10 or more years. Here's when it works, when it doesn't, and how to decide.
ReadTreatment Choices
What the 2024 Evidence Says About Root Canal Retreatment Success Rates
If a previous root canal is failing, the most useful question is no longer 'does retreatment work?' but 'in cases like mine, how well does it work, and what makes the difference?' A 2024 Journal of Endodontics systematic review of 29 studies gives the cleanest contemporary answer yet.
Read